Back to Korle Bu; Cleft Palate Surgery and Therapy- January 12th
We left Kumasi at 4:30 in the morning, and slept soundly as our expert driver and navigator led us through thick fog and heavy traffic, around familiar potholes, and past Liberian refugee camps. Our rush back to Accra was temporarily interrupted by policemen who noticed the speeding bus, but we paid the ticket “on the spot” and were back on the road on time to meet the surgical team in the Reconstructive Plastic Surgery and Burns Centre at Korle Bu Hospital. The surgical team was gracious enough to wait for our arrival to begin surgery for several cleft lip and palate patients. Our group divided into three teams based on academic and clinical experience with cleft palate, and took turns observing Dr. Paintsil, Dr. Laing, and Dr. Ampomah repairing cleft palates for an infant and then a six-year-old. 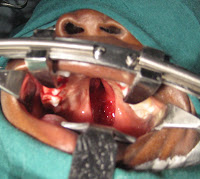
The teams from our group that were not observing surgery were upstairs providing speech, language, and feeding therapy to the cleft lip and palate patients and their families. The students saw several children of varying ages, and one adult. When evaluating the children, the students would often first ask the parent to open their mouth, and would look at it with a flashlight. After seeing their parents cooperate with the student-clinicians, the children were more comfortable and willing to show us their clefts or repairs. Many of the youngest children had already had a lip repair but were waiting for their cleft palate repair, and sessions with these children mostly consisted of feeding therapy and recommendations to encourage production of sounds that can be produced correctly even with a cleft, such as nasal sounds and vowels. 
 |
| Dr. Albert Paintsil |
 |
| Dr. Laing |
Following therapy, we participated in a cleft palate conference, held monthly, attended by the surgeons, nurses, orthodontic specialists, anesthesiologists, and other professionals such as speech- language therapists, audiologists, and Ear Nose Throat doctors. This conference was a multidisciplinary approach to treatment in full glory, with Doctors Laing, Paintsil, and Ampomah leading, and all other specialists contributing knowledge and recommendations. A student-clinician from our group presented on each patient who had been seen for therapy, and information and recommendations were shared. Recommendations included speech and language goals, as well as referrals for additional surgery, dental work, audiology appointments, and neurological evaluations. The surgeons asked us questions about our observations and recommendations, and occasionally quizzed us on our cleft palate knowledge! One important piece of information gleaned from this meeting was that our feeding recommendations had to be adapted. “In the tropics” bottle use is not encouraged, because bottles can serve as breeding grounds for bacteria due to the heat and/or poor hygiene. The students took this information into account and modified their feeding recommendations during subsequent presentations. It was a long day, and our dinner that night was the first meal we ate. But thanks to our ever-expanding knowledge base and cultural awareness, most of us already felt fulfilled.
-Charity Delsie







Thanks for your work and help bringing cleft palate surgery to the children that need it. The conference sounds like it was a great place to share ideas on cleft lips and palates.
ReplyDelete